
Supplements for ADHD: What looks promising, what may help, and what is probably overhyped
A whole-body look at saffron, pine bark extract, melatonin, omega-3s, gut-targeted supplements, vitamin D, magnesium and L-theanine, for starters…
When people ask me whether supplements help with ADHD, I rarely begin by telling them whether a supplement “works”. I start somewhere else. In fact, I may ask what, exactly, they are trying to support. Is it attention, sleep, or emotional regulation? Maybe it’s appetite, nutritional status or digestive symptoms? And then there’s the inescapable accumulated wear and tear of living in a nervous system that has had to work very hard for a very long time?
It would be much easier to say yes or no and then cite a series of studies to show off how much I have read. But, as a good ADHDer, I prefer longer answers. Sorry, not sorry! In fact, my favourite answers are the ones that make us rethink the question itself, because when the question improves, the conversation usually improves too. That’s what one of my favourite people in the world said to me once, Dr Brian Sutton - formerly Professor of Learning Performance at Middlesex, and my doctoral supervisor at Middlesex University - and it stuck with me forever. Beautiful words make the world a better place.
This matters, a lot, because ADHD is not one single “thing”. It is not just hyperactivity or inattention, so it rarely makes sense to approach it from one angle alone. In my experience, it is very easy to end up with two equally unhelpful stories. In one, supplements are dismissed completely. In the other, their effectiveness is inflated into a kind of nutritional redemption, as if capsule X could replace medication, movement, sleep, therapy, creativity, self-understanding, and the practical scaffolding so many of us genuinely need. I do not agree with either version.
So, yes, I think some supplements deserve consideration, and some are promising. But I do not think supplements replace medication or any other therapeutic approach for ADHD. The evidence base for stimulants in adults remains much stronger than the evidence base for supplements when we are talking about core ADHD symptoms. Serious and internationally respected clinical guidelines such as NICE, the National Institute for Health and Care Excellence in the UK, still recommend methylphenidate or lisdexamfetamine as first-line pharmacological treatment for adults when medication is indicated. At the same time, broader care still matters, and NICE is clear that ADHD management is not only about pharmacological treatment. ¹

What does the evidence say about saffron, omega-3s, melatonin, probiotics, magnesium and other nutritional supplements?
When I read studies on supplements, I do not simply ask whether the result is positive. I look at whether the study was done in children or adults, whether it was a pilot or a larger trial, ideally randomised and blinded, or whether it was an open-label, non-randomised study. I also think it matters whether the supplement was used as a standalone treatment or as an add-on, and what hypothesis the study was built around.
ADHD is not only about dopamine, focus and hyperactivity. From my perspective, a well-designed study should investigate the supplement’s effects on sleep, mood, behaviour and oxidative stress, as well as core ADHD symptoms. Then there’s the demographics. If a study only includes boys and not girls, or if a study only includes adult men, it becomes much harder to generalise the findings to women. These details matter far more than people often realise, because they tell us how far a finding can reasonably travel beyond the original sample.
Omega-3
Omega-3s still deserve to be part of the conversation, but the story needs to be taken with a pinch of salt, as we say in English. Fish oils, or algal oils for people who prefer not to consume animal products, are among the most researched supplements in ADHD, and that is one of the reasons they keep appearing in the conversation. The problem is that “one of the most researched” is often confused with “clearly effective”.
The Cochrane Collaboration, an independent international non-profit network that produces high-quality systematic reviews on health interventions, published an update in 2023. Its conclusion was that, overall, there was little evidence that supplementation with polyunsaturated fatty acids improved ADHD symptoms in children and adolescents. ²
A meta-analysis published that same year also found no significant overall effect on core ADHD symptoms, although longer trials, lasting at least four months, seemed somewhat more promising. In that case, the possible advantage still referred to core ADHD symptoms themselves, not to broader benefits, such as cardiovascular benefits. The study also does not allow us to say clearly which specific dimension - inattention, hyperactivity or impulsivity - benefited most. ³
That said, not all the literature points in the same direction. An earlier meta-analysis by Chang et al. found that omega-3 supplementation could modestly improve clinical ADHD symptoms and some attention-related cognitive measures in children and adolescents. It also observed that young people with ADHD tended to have lower levels of DHA, EPA and total omega-3s than controls. ⁴ This does not invalidate the more cautious reviews, but it does force us to avoid binary messages. For me, the most honest reading is that there may be a real, though small, signal, especially in children and adolescents and perhaps in longer interventions, without this justifying the presentation of omega-3s as a powerful intervention or the direct extrapolation of these findings to adults.
Omega-3s: My veredict
Omega-3s still make sense as a foundational support, with anti-inflammatory and neurobiological plausibility, but not as a strong or clearly transformative intervention by themselves.
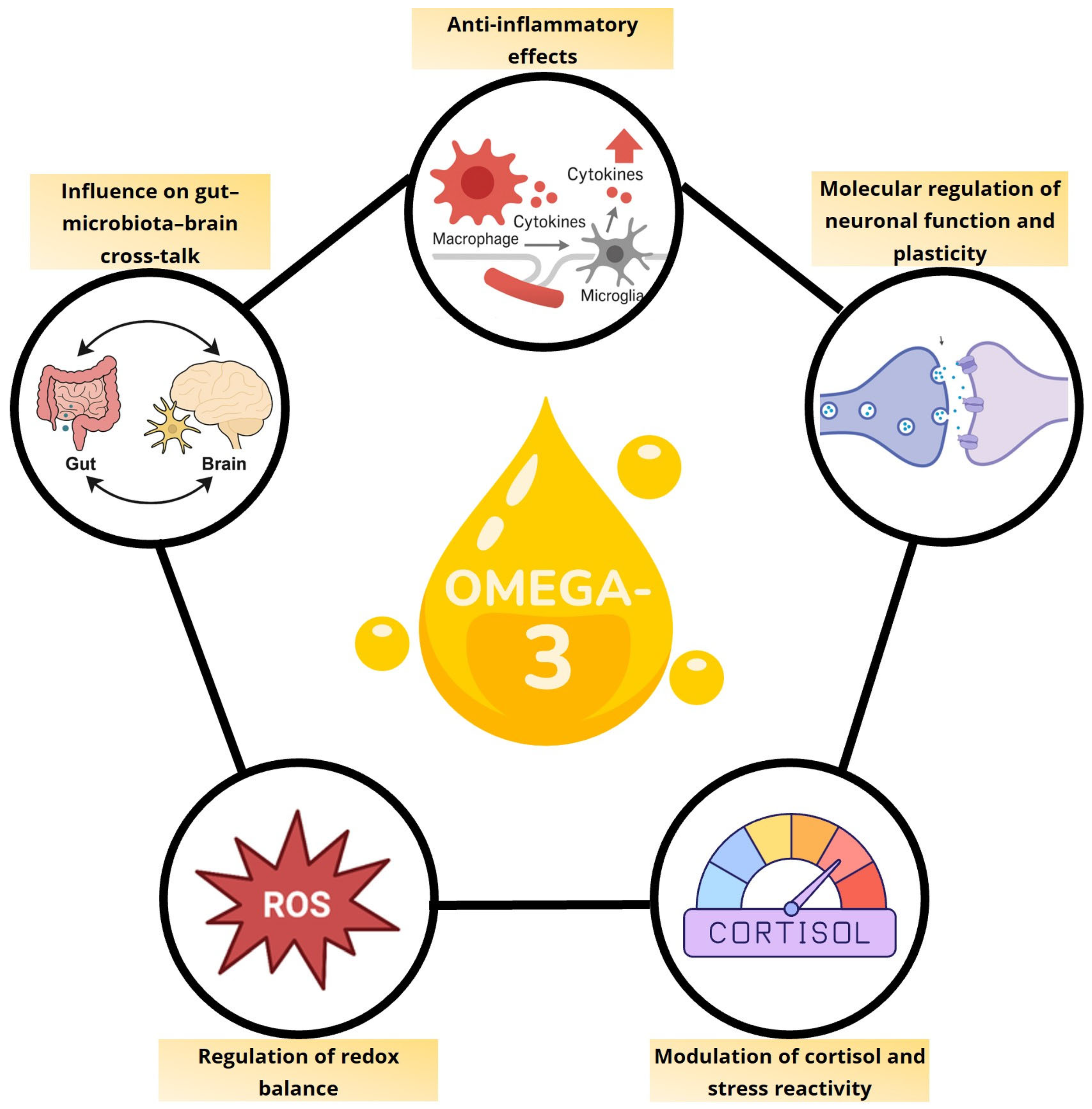
Although omega-3s do not appear to be the “miracle” for ADHD that is sometimes promised, they remain relevant nutrients because of their involvement in inflammation, oxidative stress, stress response, neuronal plasticity and the gut-microbiota-brain axis. Their value may not lie in a spectacular effect on symptoms on their own, but in their capacity to support a more regulated biological terrain, something I will explore in more detail in future articles.
Figure adapted from: De Cillis et al., Nutrients, 17(21), 3426, under a Creative Commons CC BY 4.0 licence.
Saffron
Saffron is one of the most interesting supplements in this area, and I think it deserves serious attention. But I also think it is a good example of why methodology matters.
The 2019 Baziar study is often cited because it directly compared saffron with methylphenidate in children and adolescents. ⁵ That is clinically bold and genuinely interesting, but we also need to see it for what it is: a six-week, double-blind pilot study in a small paediatric sample. A positive result in children does not automatically tell me that the same extract will behave in the same way in adults, with a different hormonal environment, other coexisting conditions, different sleep patterns, different medication exposure, and, above all, different life demands. What it tells me is that saffron deserves to be taken seriously, not that the question in adults has already been resolved.
A later study, Blasco-Fontecilla 2022, is striking for another reason. It used both objective tests and paper-and-pencil measures, which I like to see, but it was not randomised. The methylphenidate group included 27 participants and the saffron group included 36, all aged between 7 and 17. ⁶
The main finding was that saffron appeared, broadly speaking, comparable to methylphenidate, with saffron seeming stronger for hyperactivity and methylphenidate stronger for inattention. Another interesting signal, but the non-randomised design means I would be careful not to treat it as more robust than it is. Even so, the research team is excellent, and from where I stand, the study adds texture to the literature. A little like saffron adds colour to a good paella, even if it is not the main ingredient.
The adult saffron trial that feels most clinically relevant to me, precisely because it stops us leaning too heavily on child data, is the 2022 study by Pazoki and colleagues. Again, the most important detail is that this was an add-on trial. Fifty-six adults were randomly assigned to receive Ritalin with saffron or Ritalin with placebo for six weeks, and 44 completed the study. The saffron group showed a greater reduction in ASRS scores, with significant time-by-treatment effects also seen in the Conners’ Adult ADHD Rating Scales, CAARS. This does not confirm that saffron can replace stimulant treatment in adults, but it does give us an indication that methylphenidate combined with saffron may offer an interesting angle of support. It is a narrow conclusion, but an honest one. ⁷

Saffron has something especially evocative in the Spanish context, and even more so in La Mancha, where it forms part of the landscape, the cuisine and the cultural memory. Although it probably did not arrive in the Iberian Peninsula exclusively through the Arab world, it does seem clear that its expansion and deep rooting in Spain were closely linked to the Andalusian period. I like to think of this as a symbol of something wider too: how many of the things we now feel as deeply ours were actually born from exchange between cultures. Perhaps that is why saffron, as well as being beautiful and valuable, feels like a bridge between history, land and knowledge.
The adult saffron trial that feels most clinically relevant to me, precisely because it stops us leaning too heavily on child data, is the 2022 study by Pazoki and colleagues. Again, the most important detail is that this was an add-on trial. Fifty-six adults were randomly assigned to receive Ritalin with saffron or Ritalin with placebo for six weeks, and 44 completed the study. The saffron group showed a greater reduction in ASRS scores, with significant time-by-treatment effects also seen in the Conners’ Adult ADHD Rating Scales, CAARS. This does not confirm that saffron can replace stimulant treatment in adults, but it does give us an indication that methylphenidate combined with saffron may offer an interesting angle of support. It is a narrow conclusion, but at least an honest one. ⁷
In the age of AI and 15-second social media clips that cherrypick facts and present them out of context, I feel we need more honesty and less BS when interpreting science, so this is important for me. My sense of justice kicks in big time otherwise and makes me aggy 🤬
What is the ASRS?
The ASRS-v1.1, Adult ADHD Self-Report Scale, is an 18-item self-report screening questionnaire developed by the World Health Organization. It is designed to identify ADHD symptoms in adults aged 18 and over. It helps detect signs of inattention and hyperactivity/impulsivity in order to determine whether a full clinical assessment may be appropriate. On my adult ADHD screening page, you will find a free online version that you can complete to help you understand your neurotype.
The broader reviews on saffron are encouraging, but they also show how early this field still is. A 2024 systematic review of saffron in ADHD included only four studies and 118 participants in total. ⁸ Another broader 2024 review on saffron in neurological and psychiatric conditions concluded that saffron was not inferior to conventional drugs in several areas, including ADHD, but that kind of statement can sound more decisive than the ADHD dataset really allows.
My own reading is that saffron is one of the most credible options, especially when mood, sleep or emotional regulation form part of the picture, although the evidence is still limited.
Saffron: My verdict
For me, saffron is one of the most interesting and credible options in this field, especially as a well-tolerated support, although not yet as a fully established treatment for adult ADHD.

What is interesting about saffron is not only whether it improves particular symptoms, but that it seems to touch several systems at once: inflammation, neuroprotection, microbiota, the gut barrier and gut-brain signalling. In a picture as complex and embodied as ADHD, that broader biological map matters too. For these reasons, saffron continues to seem like a very interesting intervention while the evidence supporting it continues to develop.
Figure reproduced from:Cerdá-Bernad et al., Nutrients, 14(24), 5368, under a Creative Commons CC BY 4.0 licence.
As a personal anecdote, after reading these studies, I started taking saffron alongside my daily methylphenidate and I have noticed that it works better for me, with fewer peaks and troughs, in a more stable way.

Pine bark extract
Pine bark extract, usually referred to as Pycnogenol, although this is a registered trademark, is another interesting case, especially because I always find myself wondering: “Who was the first person to pulverise pine bark and give it to someone as a nutritional supplement to see what happened?” I find that both funny and amazing.
The paediatric literature on pine bark extract is broader than the adult literature. One of the earliest trials, published in 2006, included 61 children who received 1 mg/kg/day for one month. ¹⁰ Later work, including a 2021 double-blind crossover study in 20 children across two four-week phases with a two-week washout, continued to suggest possible benefits for inattention, impulsivity and oxidative balance. ¹¹
There is also a 2022 randomised trial lasting ten weeks, in which teachers reported improvements in total ADHD score and in hyperactivity or impulsivity with both pine bark extract and methylphenidate compared with placebo, while methylphenidate showed a clearer advantage for inattention. ¹²
In addition, a second analysis from the same trial explored markers of oxidative stress and immunity, as well as changes in appetite and weight. I find this interesting not because it proves one single, neat mechanism, but precisely because it reminds us that these kinds of compounds touch several physiological layers at once. At the same time, the authors themselves could not firmly confirm an overall improvement in antioxidant or immune status, so I would read this more as a clue of biological complexity than as a closed mechanistic demonstration. ¹³ My professional judgement as a researcher is that all of this deserves attention.
The adult study on pine bark extract, however, is where the question of generalisation becomes especially important. In the 2002 crossover trial, 24 adults aged between 24 and 53 received Pycnogenol, methylphenidate and placebo in randomised order, each for three weeks. ¹⁴ Although symptoms improved during treatment, neither methylphenidate nor Pycnogenol outperformed placebo on the main outcomes. That does not mean pine bark extract does nothing. It means the evidence in adults is scarce and much less clear than the evidence in children. It also means we should not move from “promising in children” to “works in adults” as if that step did not require its own evidence, although this does not deny that pine bark extract may have a range of potential benefits beyond the brain and nervous system.
Pine bark extract: My verdict
Pine bark extract is interesting not only because of what it might contribute to some symptoms, but because it points towards a broader form of support that recognises that ADHD is not lived only in the brain, but in the whole body.
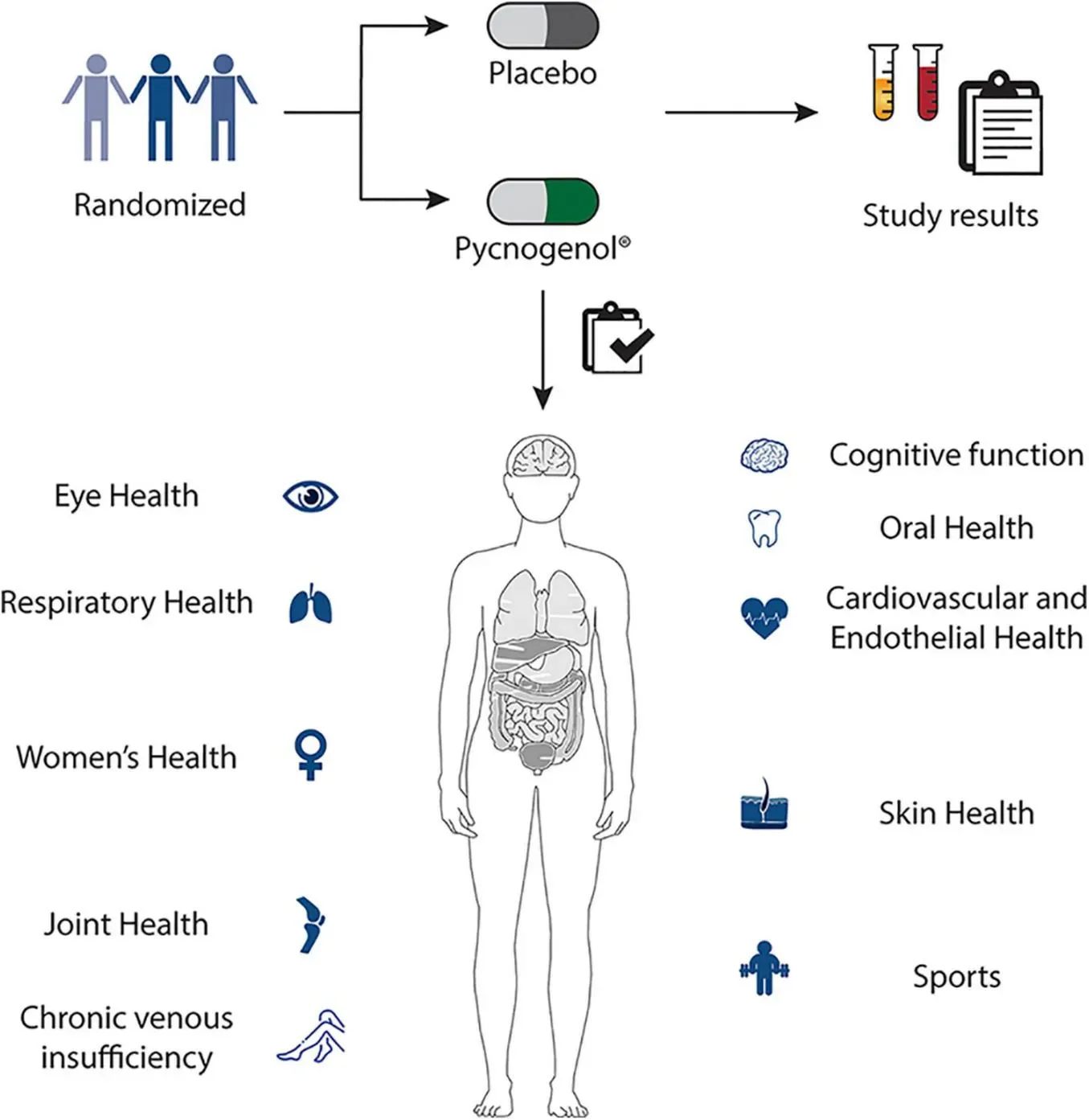
My interest in pine bark extract in ADHD is not limited to core symptoms. As with other bioactive compounds, its potential lies in the range of systems it seems to act upon, from cognitive function and vascular health to inflammatory and broader regulatory processes. In a picture as bodily as ADHD, from where I stand, that also deserves attention.
Figure adapted from: Shaw et al., Frontiers in nutrition, 11, 1389374, under a Creative Commons CC BY 4.0 licence.
Melatonin
A quick note before we begin: while melatonin is sold in many countries as a food supplement or over-the-counter sleep aid, in the UK it is a prescription-only medicine. For that reason, what follows is purely educational and is not intended as personal medical advice or a recommendation to take it.
Melatonin is best understood, in my opinion, as a support for sleep and circadian rhythm rather than as a central supplement for ADHD, and this distinction matters. In an open-label study in a small sample of children and adolescents with ADHD who were already taking psychostimulant medication, Checa-Ros and colleagues observed that a low dose of melatonin, 1 mg, was associated with an increase in total sleep time from 463 to 485 minutes over one month, alongside a trend towards improvement in other sleep variables. ¹⁵ This is a useful study, but not the type of design from which I would claim that melatonin “treats ADHD”. Rather, it suggests a possible sleep-supporting role in a specific context.
The chronotherapy work in adults is more interesting to me because it starts from the fact that adults with ADHD show greater susceptibility to delayed sleep phase syndrome. In other words, melatonin production starts later than it does in neurotypical people. Low doses of melatonin seem to advance the circadian rhythm, reducing self-reported ADHD symptoms by up to 14% immediately after supplementation, although the effect fades a few weeks after the treatment ends. ¹⁶
This tells me two things. First, that some of the suffering associated with ADHD is, in some cases, a rhythm problem. Second, that melatonin is most relevant when circadian phase delay is genuinely part of the picture, not as a universal intervention for everyone with ADHD.
The broader review on sleep interventions in children points in the same direction. Sleep interventions can improve sleep and, sometimes, ADHD-related variables, but the evidence is heterogeneous. ¹⁷ I find this review valuable because it takes us away from the reflex of thinking about sleep as secondary in ADHD. What it shows is that when sleep improves, not only can rest improve, but so can quality of life and, in some cases, aspects of the clinical picture itself. I also like it because, as a review, it does not sell clean or universal solutions. Instead, it shows a useful, promising and still quite heterogeneous field.
Melatonin: My verdict
For me, melatonin makes most sense when sleep and circadian rhythm are part of the problem, more as a regulatory support for the body-mind relationship than as a direct ADHD treatment. I take it myself and feel that it helps me rest better. This is what I think benefits me, more than any specific effect on my symptoms.
L-theanine
If we continue talking about circadian rhythms, sleep and rest, I would apply the same caution to L-theanine. I understand why it attracts so many people. It sits in that space of calm without sedation that many of us who live with ADHD are looking for, although the evidence in this field remains narrow.
In one of the best-known trials, supplementation with 400 mg daily helped improve some aspects of objective sleep quality in children with ADHD. Children, not adults, and sleep quality rather than the broader ADHD picture. ¹⁸
A 2024 systematic review of L-theanine in mental disorders also confirms that this amino acid, found in green tea, may help as an adjunct in situations where poor sleep, overstimulation or stress reactivity form part of the picture, but not as a main evidence-based treatment for adult ADHD. ¹⁹
L-theanine: My verdict
For me, L-theanine is more of a gentle support for creating a slightly calmer, more regulated and perhaps more habitable inner terrain than a primary intervention for adult ADHD.
Personally, I am very much “team L-theanine”, and I have taken it every afternoon or evening for years.
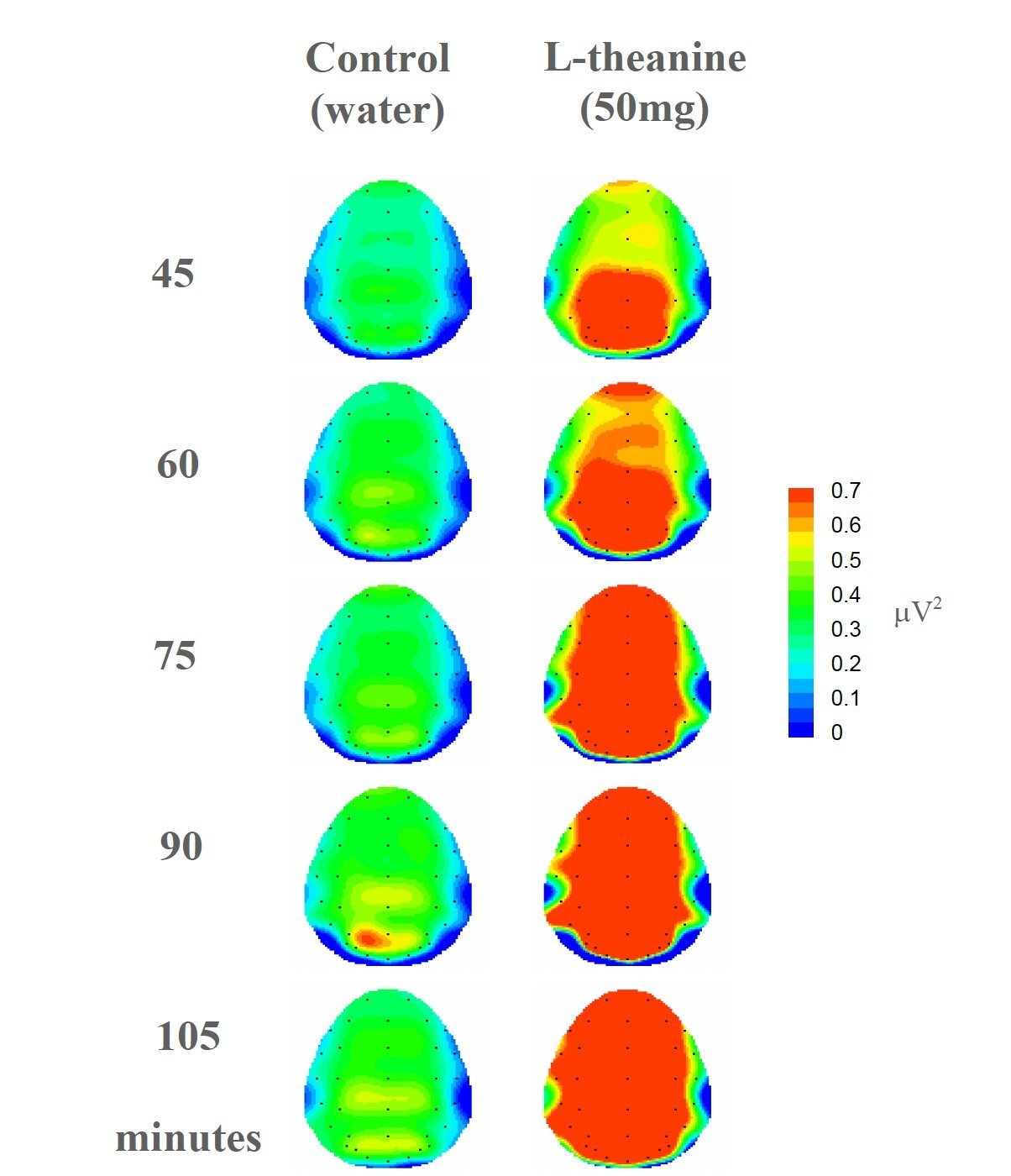
Rather than simply “calming” in a general sense, L-theanine seems to support a state of calm alertness, as reflected in the increased alpha-1 activity observed here. In a picture such as ADHD, where the problem is not always lack of activation but sometimes poorly coordinated activation, this nuance matters.
Red = more alpha-1 activity. Green = less alpha-1 activity. In this study, more red after taking L-theanine suggests a state of calm alertness, not sleepiness.
Figure adapted from: Nobre et al., Asia Pac J Clin Nutr.2008:17 Suppl 1:167-8, under a Creative Commons CC BY 4.0 licence.
Vitamin D
Vitamin D is one of those nutrients where the observational signal seems more consistent than the intervention signal. Several meta-analyses show that children and adolescents with ADHD tend to have lower serum concentrations of 25(OH)D, vitamin D3, than controls, which makes it a nutrient worth paying attention to. But that does not mean, on its own, that low vitamin D is causing ADHD in a simple and direct way.
Most of this literature is paediatric, and low levels may also reflect less time outdoors, season, adiposity, diet quality, sleep, or general health patterns that accompany ADHD, rather than clearly acting as a causal trigger. For that reason, I see it as an interesting association, but not a self-explanatory one.
The vitamin D story becomes more clinically relevant when we look at supplementation trials, although I also think the findings are sometimes overstated. The meta-analysis by Gan and colleagues, published in 2019, pooled four randomised clinical trials, including 256 children in total, and found small but statistically significant improvements in total ADHD symptoms, inattention, hyperactivity and behaviour. ²⁰
For me, however, the key methodological detail is that the studies included in this review were adjunctive trials. In other words, vitamin D was added to methylphenidate. It was not used as a standalone treatment. The authors themselves were also cautious: the evidence remained limited, and no clear improvements were seen in more challenging or oppositional behaviour problems. I would therefore read this as a modest signal of possible usefulness as an adjunct in children, not as proof that vitamin D independently “treats ADHD”.
The trial by Elshorbagy and colleagues is also striking because it reported improvements in cognitive function and in several symptom domains in children with ADHD after vitamin D supplementation. ²¹ But again, this is a paediatric study, and as with the rest of this literature, it does not resolve the question in adults. That is the point I would continue to emphasise. We still do not have robust supplementation data in adults, so it does not feel scientifically careful to extrapolate directly from child trials to adults with different physiology, more coexisting conditions such as anxiety, depression and disordered eating patterns, different medication use and different life pressures.
My current feeling is that vitamin D makes more sense as an intervention guided by nutritional status and the possibility of deficiency, especially when low levels are plausible, than as a general supplement for anyone with ADHD. The 2024 umbrella review by Kitaneh and colleagues also points in that direction: there is a plausible relationship between vitamin D and ADHD, but there is still heterogeneity and a need for better studies, especially outside paediatric populations. ²²
Vitamin D: My verdict
The way I see it, vitamin D makes more sense as a marker of physiological terrain worth checking when there are reasons to suspect low levels, rather than as a general supplement for anyone with ADHD.
Magnesium
Magnesium is a slightly different case. Here, the literature on nutritional “status” is probably more consistent than the intervention literature. Two meta-analyses found that children with ADHD tend to show lower serum magnesium levels, ²³ and one of them also observed lower levels in hair. ²⁴
Although this provides a plausible biochemical signal, the literature on magnesium is more methodologically messy than it may seem. The studies do not all measure the same thing: serum, plasma, hair, saliva, red blood cells or urine, and these matrices do not tell exactly the same story. A critical review by Robberecht and colleagues explains this point well, noting that intracellular magnesium may be a more useful indicator than serum magnesium alone, and that stimulant medication itself may influence circulating levels. ²⁵ In other words, even before talking about supplementation, the biomarker question is already less clean than some headlines suggest.
What keeps me cautious is that the supplementation literature is harder to interpret than the literature on levels. For example, the Robberecht review also notes that many magnesium trials are not “pure” magnesium trials, because the mineral was administered alongside omega-3s, zinc or other nutrients. This makes it very difficult to attribute an effect to a single component. Other studies reached similar conclusions several years ago: magnesium may help some children with ADHD, especially when there is deficiency or a high risk of deficiency, but the evidence is not strong enough to justify a routine recommendation. ²⁶
In other words, magnesium seems plausible, potentially relevant and worth assessing, but I would not yet present it as a widely evidence-backed treatment for ADHD itself.
Another important point here is the gap in adults. Most of the magnesium literature remains paediatric, and newer data in community samples are still preliminary. The 2025 article by Hunter and colleagues is useful because it tries to widen the lens beyond childhood, but it was a small, mixed sample of neurodivergent people, with only 10 adults, and not a specific ADHD intervention trial. ²⁷ This makes it valuable for generating hypotheses, but not for supporting firm treatment claims.
Magnesium: My verdict
Magnesium is really trendy at the moment. It does deserve attention mainly in an ADHD context, especially where there is restrictive eating, sensory selectivity, poor sleep, chronic stress or lower intake, but only as a string to a multi-string bow, rather than as a specific treatment for ADHD itself.

Would you like to know more about magnesium-rich foods? Read this article from Healthline: 10 Magnesium-Rich Foods That Are Super Healthy.
The gut microbiome, probiotics and fermented foods
The literature on the gut and brain is fascinating, but this is one of the easiest areas to exaggerate. And believe me, because this is the field I have been working in for many years, and I increasingly hear and read a lot of nonsense with very little scientific basis.
The 2024 systematic review by Allahyari and colleagues concluded that probiotics and prebiotics may be beneficial as adjunctive therapies in ADHD, but also called for longer studies, with more participants, a wider age range and more varied assessment methods. ²⁸ That feels like a fair summary of where we are. There is promise, but there is still a lot we do not know.
Data in adults remain especially scarce. A good example is a 2025 systematic review on gut microbiota modulation in adults with ADHD, which ended up including only three randomised clinical trials. ²⁹ Among those studies, the double-blind adult trial by Schwartz and colleagues, published in 2024, is especially interesting because it reported less hyperactivity, fewer gastrointestinal symptoms and better academic performance after probiotic intervention, with younger age being one of the predictors of a more favourable response. ³⁰
That said, when we talk about the microbiota, not everything has to be reduced to a probiotic capsule. In my own research, I have also explored microbiota-targeted interventions through diet and fermented foods such as kefir. I am especially interested in this approach because it moves away from the idea of a miracle strain and closer to a lived, edible and potentially more integrated intestinal ecology.
First, we published a feasibility study in Pilot and Feasibility Studies, where we tested a microbiome-targeted dietary intervention in children with ADHD and observed that the approach was safe, tolerable and feasible, with good adherence and enough signal to justify a larger trial. ³¹ We then published the protocol for the randomised trial on kefir, behaviour, sleep and the microbiome in BMJ Open, precisely to study this kind of food-based intervention more rigorously. ³² More recently, the clinical trial results were published in BMC Psychiatry. ³³
I do not think these studies close the case, not at all, but they do help widen the conversation. Perhaps the future of this field does not lie only in isolated supplements, but also in broader, more food-based ways of modulating the gut-brain axis.
Probiotics: My verdict
With my gut-brain axis and mental health researcher hat on, this is a very promising and biologically fascinating field, but still too random and preliminary for us to talk about universal solutions. The most interesting thing may not be one specific strain, but a more ecological and food-based way of working on the health of the communication between gut and brain/nervous system.
In the end, a tool, not a solution
All of this is one of the reasons I keep returning to the bigger picture. A capsule can support one layer of the system, but however tempting it may be, or however much it is sold to you as part of a “premium protocol”, it can never be the whole system.
Let me give you a brief example to illustrate what I mean. Movement matters, not simply because exercise is “healthy”, but because it changes physiology in ways that are relevant for regulation. Recent reviews suggest that exercise may increase microbial diversity in adults, enhance short-chain fatty acid production, and support adaptation and mitochondrial biogenesis. ³⁴ ³⁵ In other words, movement is not only about muscles. It is about energy, gut-brain signalling and state change. That is a very different conversation, and a much truer one, than “go for a run and your ADHD will be fixed”.
So, with all this caution, where does it leave us? From where I write, I may sound cautious, yes, but I can assure you that I also feel hopeful. I think saffron is worth watching closely. I think pine bark extract is very interesting, especially in younger ADHDers. I think melatonin can be very relevant when nervous system dysregulation affects sleep timing. I also think vitamin D and magnesium make more sense when low levels are plausible, and that L-theanine may help some people, especially in relation to overstimulation. And, of course, having specialised in the microbiota and mental health, I find this field fascinating, although I must recognise that it is still young.
Above all, I think supplements can support a broader plan, but they cannot be the plan. And I say that as a researcher, as a clinician and as a neurodivergent person who has spent many years trying almost everything.
So, to finish, I do not think the question is “which supplement fixes ADHD?” but “what needs support in my body and mind, and what can this tool realistically contribute?” It is a less flashy question, but a much more useful one, because it leaves enough space for medication, therapy, food, movement, creativity and self-compassion to form part of the same conversation, which is where I think they belong.
With care,

The content of this article is for educational and informational purposes only. It is not intended to replace medical advice, diagnosis, psychotherapy or individualised treatment from a qualified professional. If you are making decisions about medication, supplements, mental health, sleep or any other aspect of your care, please speak with your doctor, prescriber and/or therapist first.
If you are trying to decide more clearly what role supplements, food, medication or other forms of support may have in your specific case, my ADHD & Neurodivergence Wellbeing page explains how I work one-to-one.
Important note: This review comes from my professional and research interests in the field, as well as my educational and clinical experience. If you are considering any of these supplements in the context of a medical condition or pharmacological treatment, please discuss this first with your doctor or a qualified dietitian or nutrition professional.
Please note also that melatonin is prescription-only in certain countries, including the UK, so please consult with your doctor if you’re thinking of taking it and are unsure of whether it’d be appropriate in your particular case.
References: The science informing this article
National Institute for Health and Care Excellence. (2018, actualizado 2019). Attention deficit hyperactivity disorder: Diagnosis and management (NICE Guideline NG87).https://www.nice.org.uk/guidance/ng87
Notes: This NICE clinical guideline from the UK sets out evidence-based recommendations for ADHD diagnosis and treatment across the lifespan. It highlights that pharmacological treatment, including methylphenidate and lisdexamfetamine in adults, should be integrated within a broader and personalised therapeutic plan.
Gillies, D., Leach, M. J., & Perez Algorta, G. (2023). Polyunsaturated fatty acids (PUFA) for attention deficit hyperactivity disorder (ADHD) in children and adolescents. The Cochrane database of systematic reviews, 4(4), CD007986. https://doi.org/10.1002/14651858.CD007986.pub3
Notes: This study matters because it acts as a necessary counterweight to the enthusiasm that tends to surround omega-3s in ADHD. As a Cochrane review, it offers a particularly rigorous and cautious reading of the evidence available in children and adolescents, and reminds us that “widely researched” is not the same as “clearly effective”. In the context of this article, it helps place omega-3s in a more honest position: as a potential support within a broader approach, not as a powerful solution or something easily extrapolated to adults.
Liu, T.-H., Wu, J.-Y., Huang, P.-Y., Lai, C.-C., Chang, J. P.-C., Lin, C.-H., & Su, K.-P. (2023). Omega-3 polyunsaturated fatty acids for core symptoms of attention-deficit/hyperactivity disorder: A meta-analysis of randomized controlled trials. Journal of Clinical Psychiatry, 84(5), 22r14772. https://doi.org/10.4088/JCP.22r14772
Notes: What is interesting about this meta-analysis is that the possible advantage of omega-3s appeared only in longer trials, lasting at least four months, and referred to core ADHD symptoms overall as a modest signal within the ADHD clinical picture itself. At the same time, the study does not allow us to say clearly which specific dimension, inattention, hyperactivity or impulsivity, benefited most from longer duration.
Chang, J. P., Su, K. P., Mondelli, V., & Pariante, C. M. (2018). Omega-3 Polyunsaturated Fatty Acids in Youths with Attention Deficit Hyperactivity Disorder: a Systematic Review and Meta-Analysis of Clinical Trials and Biological Studies. Neuropsychopharmacology : official publication of the American College of Neuropsychopharmacology, 43(3), 534–545. https://doi.org/10.1038/npp.2017.160
Notes: Chang et al. is important because it introduces a necessary nuance into a literature that, if viewed only through more recent reviews, might seem more negative than it really is. Its value lies in detecting a favourable signal in children and adolescents, both in clinical symptoms and in some attention measures, while also adding biological plausibility by showing lower DHA and EPA levels in young people with ADHD. This study supports a balanced position: omega-3s do not seem to be a powerful intervention, but they cannot be dismissed as irrelevant either, especially in younger populations and perhaps in longer trials.
Baziar, S., Aqamolaei, A., Khadem, E., Mortazavi, S. H., Naderi, S., Sahebolzamani, E., Mortezaei, A., Jalilevand, S., Mohammadi, M. R., Shahmirzadi, M., & Akhondzadeh, S. (2019). Crocus sativus L. Versus Methylphenidate in Treatment of Children with Attention-Deficit/Hyperactivity Disorder: A Randomized, Double-Blind Pilot Study. Journal of child and adolescent psychopharmacology, 29(3), 205–212. https://doi.org/10.1089/cap.2018.0146
Notes: This study is important because it was one of the first trials to directly compare saffron and methylphenidate in children with ADHD, using a randomised, double-blind design. Its main interest lies in suggesting possible comparable short-term efficacy, but because it was a pilot study, with a small sample and only in children and adolescents, its results should be read as a promising signal, not as definitive proof or something easily extrapolated to adults. That is why I insist that methodology and sample demographics are always key if we want to avoid exaggerating the results of a study, however promising it may look.
Blasco-Fontecilla, H., Moyano-Ramírez, E., Méndez-González, O., Rodrigo-Yanguas, M., Martin-Moratinos, M., & Bella-Fernández, M. (2022). Effectivity of Saffron Extract (Saffr'Activ) on Treatment for Children and Adolescents with Attention Deficit/Hyperactivity Disorder (ADHD): A Clinical Effectivity Study. Nutrients, 14(19), 4046. https://doi.org/10.3390/nu14194046
Notes: A suggestive study because it explores the potential of saffron in children and adolescents with ADHD and includes more objective measures than many similar studies. Even so, its non-randomised design means it must be interpreted cautiously: it provides an interesting signal, but not definitive proof, and not something easily extrapolated to adults. Safety may warrant experimentation, but your expectations should be commensurate with the quality of the evidence available.
Pazoki, B., Zandi, N., Assaf, Z., Sanjari Moghaddam, H., Zeinoddini, A., Mohammadi, M. R., & Akhondzadeh, S. (2022). Efficacy and safety of saffron as adjunctive therapy in adults with attention-deficit/hyperactivity disorder: A randomized, double-blind, placebo-controlled clinical trial. Advances in Integrative Medicine, 9(1), 37–43. https://doi.org/10.1016/j.aimed.2022.01.002
Notes: This study feels especially relevant to me because it moves the conversation on saffron from childhood into the adult population, which remains uncommon in this field. It also does not evaluate saffron as a substitute for medication, but as an add-on to methylphenidate, which makes the clinical question more realistic. Its main value is that it offers a promising signal in adults within a randomised, double-blind, placebo-controlled design. At the same time, it remains a small and short study, so I would read it as an interesting proof of concept, not as definitive confirmation of efficacy.
Seyedi-Sahebari, S., Farhang, S., Araj-Khodaei, M., Akhondzadeh, S., Naseri, A., Sanaie, S., & Frounchi, N. (2024). The Effects of Crocus sativus (Saffron) on ADHD: A Systematic Review. Journal of Attention Disorders, 28(1), 14–24. https://doi.org/10.1177/10870547231203176
Notes: A small review, yes, but useful precisely because of that. It reminds us that enthusiasm for saffron in ADHD still rests on a handful of studies, not a mountain of evidence. Promising, yes; mature, not yet. But with tolerability that, so far, seems reasonably good. And as an intervention based on a food traditionally used for centuries, if expectations are appropriate, it may be a relatively low-risk way to experiment.
Han, S., Cao, Y., Wu, X., Xu, J., Nie, Z., & Qiu, Y. (2024). New horizons for the study of saffron (Crocus sativus L.) and its active ingredients in the management of neurological and psychiatric disorders: A systematic review of clinical evidence and mechanisms. Phytotherapy Research : PTR, 38(5), 2276–2302. https://doi.org/10.1002/ptr.8110
Notes: This review is interesting because it broadens the focus considerably and places ADHD within a wider clinical map. For precisely that reason, it needs to be read carefully: when the zoom is pulled back too far, the ADHD-specific detail can seem more solid than it really is.
Trebatická, J., Kopasová, S., Hradecná, Z., Cinovský, K., Skodácek, I., Suba, J., Muchová, J., Zitnanová, I., Waczulíková, I., Rohdewald, P., & Duracková, Z. (2006). Treatment of ADHD with French maritime pine bark extract, Pycnogenol. European child & adolescent psychiatry, 15(6), 329–335. https://doi.org/10.1007/s00787-006-0538-3.
Notes: This trial has almost historical value within this small niche, because it helped put pine bark extract on the ADHD map long before the topic became “fashionable”. It is also interesting that even then, it pointed towards oxidative stress as part of the picture, something that today fits quite well with more systemic and less reductionist readings of ADHD, where inflammation and oxidative stress are considered potentially relevant layers.
Hsu, C. D., Hsieh, L. H., Chen, Y. L., Lin, I. C., Chen, Y. R., Chen, C. C., Shirakawa, H., & Yang, S. C. (2021). Complementary effects of pine bark extract supplementation on inattention, impulsivity, and antioxidative status in children with attention-deficit hyperactivity disorder: A double-blinded randomized placebo-controlled cross-over study. Phytotherapy Research: PTR, 35(6), 3226–3235. https://doi.org/10.1002/ptr.7036
Notes: The most appealing aspect of this study is not only the crossover design, which allows each child to act partly as their own control, but also the attempt to connect behaviour and antioxidant status in the same work. I see it as a good example of an intuition running through this whole article: sometimes the most interesting changes do not happen at one single level, but in the conversation between symptoms, biology and context.
Weyns, A.-S., Verlaet, A. A. J., Breynaert, A., Naessens, T., Fransen, E., Verhelst, H., Van West, D., Van Ingelghem, I., Jonckheere, A. I., Beysen, D., Kenis, S., Moens, E., van Roest, A. P. J., Savelkoul, H. F. J., De Bruyne, T., Pieters, L., Ceulemans, B., & Hermans, N. (2022). Clinical investigation of French maritime pine bark extract on attention-deficit hyperactivity disorder as compared to methylphenidate and placebo: Part 1: Efficacy in a randomised trial. Journal of Functional Foods, 97, 105246. https://doi.org/10.1016/j.jff.2022.105246
Notes: This study is particularly useful because it introduces a more demanding comparison than usual: not only against placebo, but also against methylphenidate. That forces pine bark extract into a more clinical and less idealised space. It does not make it a substitute for anything, but it does move it out of the purely speculative drawer.Weyns, A.-S., Verlaet, A. A. J., Van Herreweghe, M., Breynaert, A., Fransen, E., De Meester, I., Logie, E., Vanden Berghe, W., Verhelst, H., Van West, D., Van Ingelghem, I., Jonckheere, A. I., Beysen, D., Kenis, S., Moens, E., van Roest, A. P. J., Savelkoul, H. F. J., De Bruyne, T., Pieters, L., Ceulemans, B., & Hermans, N. (2022). Clinical investigation of French maritime pine bark extract on attention-deficit hyperactivity disorder as compared to methylphenidate and placebo: Part 2: Oxidative stress and immunological modulation. Journal of Functional Foods, 97, 105247. https://doi.org/10.1016/j.jff.2022.105247
Notes: I like this second article by Weyns and colleagues because it complicates the story, and as a good ADHDer, I love a complicated story! In this case, making it more complicated is a virtue. Instead of confirming a neat and elegant mechanism, it shows how difficult it is to robustly demonstrate that a compound acts exactly where we suspect it might act. Biology is often more tangled and less elegant than the hypotheses scientists create, and precisely for that reason, it feels more believable.Tenenbaum, S., Paull, J. C., Sparrow, E. P., Dodd, D. K., & Green, L. (2002). An experimental comparison of Pycnogenol and methylphenidate in adults with Attention-Deficit/Hyperactivity Disorder (ADHD). Journal of attention disorders, 6(2), 49–60. https://doi.org/10.1177/108705470200600201.
Notes: This study is important because it is one of the few trials looking at pine bark extract in adults with ADHD. Its findings were not particularly convincing, since neither Pycnogenol nor methylphenidate clearly outperformed placebo on the main outcomes. For me, that does not mean pine bark extract should be dismissed entirely, but it does remind us that adult evidence is still scarce, and that promising findings in children cannot simply be carried over into adult ADHD without proper studies.
Checa-Ros, A., Muñoz-Hoyos, A., Molina-Carballo, A., Viejo-Boyano, I., Chacín, M., Bermúdez, V., & D'Marco, L. (2023). Low Doses of Melatonin to Improve Sleep in Children with ADHD: An Open-Label Trial. Children (Basel, Switzerland), 10(7), 1121. https://doi.org/10.3390/children10071121
Notes: I find this study useful because it focuses on something that often gets pushed into the background in ADHD: sleep. It also reminds us that improving rest can be clinically relevant even when we are not directly “treating ADHD”. Because this was an open-label study, in a small paediatric sample already taking psychostimulant medication, I would read it as an interesting early signal, more useful for opening good questions than for closing conclusions.van Andel, E., Bijlenga, D., Vogel, S. W. N., Beekman, A. T. F., & Kooij, J. J. S. (2021). Effects of chronotherapy on circadian rhythm and ADHD symptoms in adults with attention-deficit/hyperactivity disorder and delayed sleep phase syndrome: a randomized clinical trial. Chronobiology international, 38(2), 260–269. https://doi.org/10.1080/07420528.2020.1835943
Notes: I find this study especially valuable because it shifts the conversation away from “attention deficit” and towards something much more basal and embodied: circadian rhythm. In adults with ADHD and delayed sleep phase syndrome, it reminds us that sometimes part of the suffering is not only about attention itself, but about living physiologically out of sync. I also like that it does not present chronotherapy as a magic solution, but as an interesting way of thinking about ADHD through time, sleep and regulation, something I discuss in my book ADHD Body and Mind.Larsson, I., Aili, K., Lönn, M., Svedberg, P., Nygren, J. M., Ivarsson, A., & Johansson, P. (2023). Sleep interventions for children with attention deficit hyperactivity disorder (ADHD): A systematic literature review. Sleep medicine, 102, 64–75. https://doi.org/10.1016/j.sleep.2022.12.021
Notes: This is a particularly useful review because it reminds us that intervening on sleep is not “treating something separate”, but working on a very relevant layer for those of us who live with ADHD. Its main strength lies in bringing some order to a promising field that is still uneven and somewhat tangled in terms of methods and results.Lyon, M. R., Kapoor, M. P., & Juneja, L. R. (2011). The effects of L-theanine (Suntheanine®) on objective sleep quality in boys with attention deficit hyperactivity disorder (ADHD): a randomized, double-blind, placebo-controlled clinical trial. Alternative medicine review : a journal of clinical therapeutic, 16(4), 348–354.
Notes: I find this study interesting because it places L-theanine in a more realistic and, for me, more useful position: not so much as a broad “ADHD supplement”, but as a possible support for one specific layer of the picture, sleep. It also reminds us of something important in this article: sometimes improving rest does not resolve ADHD, but it can soften the experience of living with it. I have been taking 400 mg every afternoon/evening for some time.Moshfeghinia, R., Sanaei, E., Mostafavi, S., Assadian, K., Sanaei, A., & Ayano, G. (2024). The effects of L-theanine supplementation on the outcomes of patients with mental disorders: a systematic review. BMC psychiatry, 24(1), 886. https://doi.org/10.1186/s12888-024-06285-y
Notes: I find this review useful because it places L-theanine in a more realistic role: not as a star solution, but as a gentle and potentially interesting support in pictures where anxiety, overstimulation or poor sleep form part of the problem. It also usefully reminds us that we need to be quite cautious when extrapolating from “mental disorders” in general to adult ADHD.Gan, J., Galer, P., Ma, D., Chen, C. y Xiong, T. (2019). The Effect of Vitamin D Supplementation on Attention-Deficit/Hyperactivity Disorder: A Systematic Review and Meta-Analysis of Randomized Controlled Trials. Journal of Child and Adolescent Psychopharmacology, 29(9), 670–687.
Notes: This is an important meta-analysis because it helps ground the conversation around vitamin D. There is a small favourable signal, yes, but in paediatric trials and as an add-on to methylphenidate, not as an independent treatment. Its main value lies in forcing us to distinguish between a plausible adjunctive support and a primary intervention, which would be saying too much.
Elshorbagy, H.H., Barseem, N.F., Abdelghani, W.E. et al. (2018). Impact of Vitamin D Supplementation on Attention-Deficit Hyperactivity Disorder in Children. Annals of Pharmacotherapy, 52(7), 623–631.
Notes: This study is interesting because it points to cognitive and behavioural improvements after vitamin D supplementation in children, but also because it illustrates one of the recurring limits in this field: the findings are suggestive in paediatric populations, without resolving the bigger question of whether something similar happens in adults. It opens a door, but it does not close the debate.Kitaneh, R., Jalilian-Khave, L., Ysrayl, B.B. et al. (2024). The Relationship Between Vitamin D and the Development and Treatment of Attention-Deficit Hyperactivity Disorder: An Overview of Systematic Reviews. Current Behavioral Neuroscience Reports, 11(3), 164–181.
Notes: I find this umbrella review especially useful because it does not try to simplify a literature that remains quite heterogeneous. Rather than selling a firm conclusion, it helps place vitamin D where it probably belongs right now: as a biologically plausible and clinically interesting factor, but still far from justifying excessive enthusiasm.Effatpanah, M., Rezaei, M., Effatpanah, H. et al. (2019). Magnesium status and attention deficit hyperactivity disorder (ADHD): A meta-analysis. Psychiatry Research, 274, 228–234.
Notes: This is a useful meta-analysis because it reinforces the idea that magnesium deserves attention as a biological marker, although not necessarily as a therapeutic solution in itself. It is also a good warning against rushed interpretations: the signal exists, but the heterogeneity between studies remains too high to draw simplistic conclusions.Huang, Y.H., Zeng, B.Y., Li, D.J. et al. (2019). Significantly lower serum and hair magnesium levels in children with attention deficit hyperactivity disorder than controls: A systematic review and meta-analysis. Progress in Neuro-Psychopharmacology and Biological Psychiatry, 90, 134–141.
Notes: What I find most valuable about this review is that it expands the conversation beyond serum and also includes hair levels, reminding us that “magnesium status” cannot always be captured by a single biomarker. It provides a consistent signal in children, yes, but it also makes clear that measuring something is not the same as knowing exactly what to do clinically with that information. The value lies in translating these data into clinical intervention, but we still need more clarity.Robberecht, H., Verlaet, A.A.J., Breynaert, A., De Bruyne, T. y Hermans, N. (2020). Magnesium, Iron, Zinc, Copper and Selenium Status in Attention-Deficit/Hyperactivity Disorder (ADHD). Molecules, 25(19), 4440.
Notes: I like this review because it introduces a much-needed layer of complexity. Instead of assuming that “low in blood” automatically means “clinical deficiency” or “needs supplementation”, it reminds us that mineral biomarkers tell partial and sometimes contradictory stories. In a field so prone to being simplified on social media, nuance matters. Science is not always easy to turn into Instagram stories.Lange, K.W., Hauser, J., Lange, K.M. et al. (2017). The Role of Nutritional Supplements in the Treatment of ADHD: What the Evidence Says. Current Psychiatry Reports, 19(2), 8.
Notes: This is a particularly useful review article as a general map, because it brings some order to an area where biological plausibility can easily be confused with proven clinical efficacy. Its cautious tone remains very relevant: some nutrients may help in specific contexts, but the evidence is far from supporting broad promises or easy solutions.Hunter, C., Smith, C., Davies, E., Dyall, S.C. y Gow, R.V. (2025). A closer look at the role of nutrition in children and adults with ADHD and neurodivergence. Frontiers in Nutrition, 12, 1586925.
Notes: I find this paper interesting because it tries to open the nutritional conversation beyond childhood ADHD alone, incorporating adults and other forms of neurodivergence too. Precisely because of that, it should be read as what it is: a preliminary piece, useful for generating questions and detecting patterns, but not for supporting strong clinical claims by itself. It is certainly not a paper we can use to create a “nutritional protocol for ADHD”.Allahyari, P., Abbas Torki, S., Aminnezhad Kavkani, B., Mahmoudi, Z., Mousavi Hoseini, M. S., Moradi, M., Alami, F., Keshavarz Mohammadian, M., Bahoo Sele Bani, S., Abbasi Mobarakeh, K., Shafaei, H., Khoshdooz, S., Hajipour, A., Doaei, S., & Gholamalizadeh, M. (2024). A systematic review of the beneficial effects of prebiotics, probiotics, and synbiotics on ADHD. Neuropsychopharmacology reports, 44(2), 300–307. https://doi.org/10.1002/npr2.12437
Notes: This is a useful review because it summarises the current state of the field well: there are promising signals, but still too much entanglement around strains, duration, age and outcome measures for us to speak with excessive confidence. In other words, interesting, yes; ready for commercial simplification, no.Gomes, A., Soares, A., Correia, C. G., Castelo-Branco, M., & Oliveira, G. (2025). The effectiveness of the gut microbiota modulation on ADHD in adults: A systematic review. Current Developmental Disorders Reports. Advance online publication. https://doi.org/10.1007/s40501-025-00358-9
Notes: I find this review very valuable precisely because it lowers the volume of the enthusiasm. In adults with ADHD, the field is still so small that a systematic review ends up working with only three randomised trials. Sometimes the most important finding of a review is not what it confirms, but how little we still know.Levy Schwartz, M., Magzal, F., Yehuda, I., & Tamir, S. (2024). Exploring the impact of probiotics on adult ADHD management through a double-blind RCT. Scientific reports, 14(1), 26830. https://doi.org/10.1038/s41598-024-73874-y
Notes: For me, this is one of the most interesting adult studies, not because it resolves the topic, but because it connects ADHD symptoms, gastrointestinal symptoms and functional performance within the same trial. I also like that it found a more favourable response in younger participants, because it suggests that the story may not only be about “whether it works”, but also about when, in whom and under what conditions. The nuances are what I find most fascinating as science unfolds in fields as complex as this one.Lawrence, K., Myrissa, K., Toribio-Mateas, M., Minini, L., & Gregory, A. M. (2022). Trialling a microbiome-targeted dietary intervention in children with ADHD: the rationale and a non-randomised feasibility study. Pilot and feasibility studies, 8(1), 108. https://doi.org/10.1186/s40814-022-01058-4
Notes: For me, this study has value because it shifts the focus from an isolated supplement towards a microbiota-targeted dietary intervention. It does not try to prove spectacular efficacy too early. It does something more important at the beginning of a research programme: it checks whether the approach is feasible, safe and reasonably liveable in real life. I am also one of the authors, and it was an enriching experience to work on the study design, implementation and interpretation of the data.Lawrence, K., Fibert, P., Hobbs, J., Myrissa, K., Toribio-Mateas, M. A., Quadt, F., Cotter, P. D., & Gregory, A. M. (2023). Randomised controlled trial of the effects of kefir on behaviour, sleep and the microbiome in children with ADHD: a study protocol. BMJ open, 13(12), e071063. https://doi.org/10.1136/bmjopen-2022-071063
Notes: Although this is a protocol, I find it an important reference because it shows methodological ambition and conceptual clarity. It presents kefir not simply as a “natural probiotic”, but as a complex food-based intervention with the potential to influence behaviour, sleep and the microbiome within a more rigorous design. I am also one of the authors, and the reason it was published is important. We learned a great deal in our preliminary study, which meant we needed to be transparent with the scientific community and acknowledge that some of our assumptions were not correct, and that the methods we had used in the feasibility study were not the most appropriate.Lawrence, K., Fibert, P., Toribio-Mateas, M., Gregory, A. M., Hobbs, J., Quadt, F., Wright, S., Cotter, P. D., Patel, S., & Myrissa, K. (2025). Effects of kefir on symptoms, sleep, and gut microbiota in children with ADHD: a randomised controlled trial. BMC psychiatry, 25(1), 1117. https://doi.org/10.1186/s12888-025-07568-8
Notes: I find this trial especially valuable because it allowed us to take the conversation one step beyond the “probiotic pill mindset” and study a whole fermented food in a controlled trial. What interests me most is not selling kefir as a solution, but opening a more ecological and food-based route for thinking about gut-brain axis modulation in ADHD. I am very proud of the work my colleagues and I did, and of having been able to publish it in such an eminent psychiatry journal.Min, L., Ablitip, A., Wang, R., Luciana, T., Wei, M., & Ma, X. (2024). Effects of Exercise on Gut Microbiota of Adults: A Systematic Review and Meta-Analysis. Nutrients, 16(7), 1070. https://doi.org/10.3390/nu16071070
Notes: I find this review useful because it reinforces one of the central ideas in this article: movement does not only benefit muscle or mood, it also seems to dialogue with intestinal ecology. I have to be honest and say that it does not turn exercise into a panacea, but it does help us think about the body as a network of systems with the potential to influence and benefit one another.Al-Beltagi, M., Saeed, N. K., Bediwy, A. S., El-Sawaf, Y., Elbatarny, A., & Elbeltagi, R. (2025). Exploring the gut-exercise link: A systematic review of gastrointestinal disorders in physical activity. World journal of gastroenterology, 31(22), 106835. https://doi.org/10.3748/wjg.v31.i22.106835
Notes: I find this review interesting because it expands the conversation between exercise and the gut beyond the isolated microbiota and places it within a more global physiology. In the context of this article, it helps support the idea that movement affects much more than energy expenditure, modifying the bodily terrain from which we live ADHD.
Join the conversation
Share a thought, reflection or question.
Please keep this space thoughtful, respectful and kind. Thank you.