
ADHD meds: Goal, or breathing space?
There is a very understandable fantasy that often appears when we finally receive an ADHD diagnosis. The fantasy that now, at last, a pill will put all the pieces in their place. That you will finally do everything you have spent years wanting to do. That the noise will go quiet. That the anguish will disappear. That life, finally, will begin to feel lighter.
I understand this. I really do.
But I think that expectation, although deeply human, can hurt us. Because ADHD medication can be very useful. Sometimes it is so useful that it can change your life within days. But if we receive it as something passive, as if it were a perfect solution that acts on us while we continue waiting somewhere outside ourselves, it can fall short.
It may help you concentrate better, start tasks, feel more mental clarity and even improve your quality of life in measurable ways. But on its own, it does not usually touch the existential anguish you may have been living with since childhood. That sense of being late, of letting yourself down, of not managing, of not understanding why life can feel so uphill. ¹ ² ³
This actually fits quite well with how serious clinical guidelines now understand treatment. NICE, the National Institute for Health and Care Excellence in the UK, does not frame adult ADHD treatment as an isolated decision, but as part of a comprehensive and shared plan that takes into account your goals, your everyday functioning, your sleep, and your psychological, behavioural and occupational needs. Within that framework, methylphenidate and lisdexamfetamine remain among the first-line pharmacological options for adults, because they have real efficacy for core symptoms such as hyperactivity, impulsivity, and the peaks and troughs of attention.

Medication does not create a new version of you
Medication does not turn you into someone else or create concentration from nothing. What it does, neurobiologically, is increase the availability of dopamine and noradrenaline and support the functioning of brain networks involved in attention, motivation and impulse control. In other words, it does not give you a new life, but it can give you something just as valuable: breathing space. Less noise, less friction and less wasted effort.
For me, as someone who lived without a diagnosis until the age of 47, that breathing space matters far more than we often recognise.
Because the benefit is not only becoming more productive. In fact, I like to think about it differently, and I would say that productivity is far too narrow a way to understand what medication can offer. The benefit, most of the time, if you ask someone who has been helped by medication, is feeling less guilt, less accumulated shame at the end of the day, less distance between what you wanted to do and what you were finally able to hold. Less of that feeling of secretly failing at tasks that, from the outside, seem simple for everyone except you.
That is the point where, for me, medication starts to become really interesting. Not when it turns you into a performance machine, but when it reduces enough friction for you to begin relating to yourself with more tenderness and less punishment.
Because if there is one thing I have learned, it is that pharmacological treatment truly shines when it meets self-awareness. When you do not use it to obey toxic productivity more efficiently, but to move closer to who you are. When the diagnosis does not become a static label, but an invitation to ask yourself honestly: what do I need in order to live with more coherence, more presence and less internal tension?
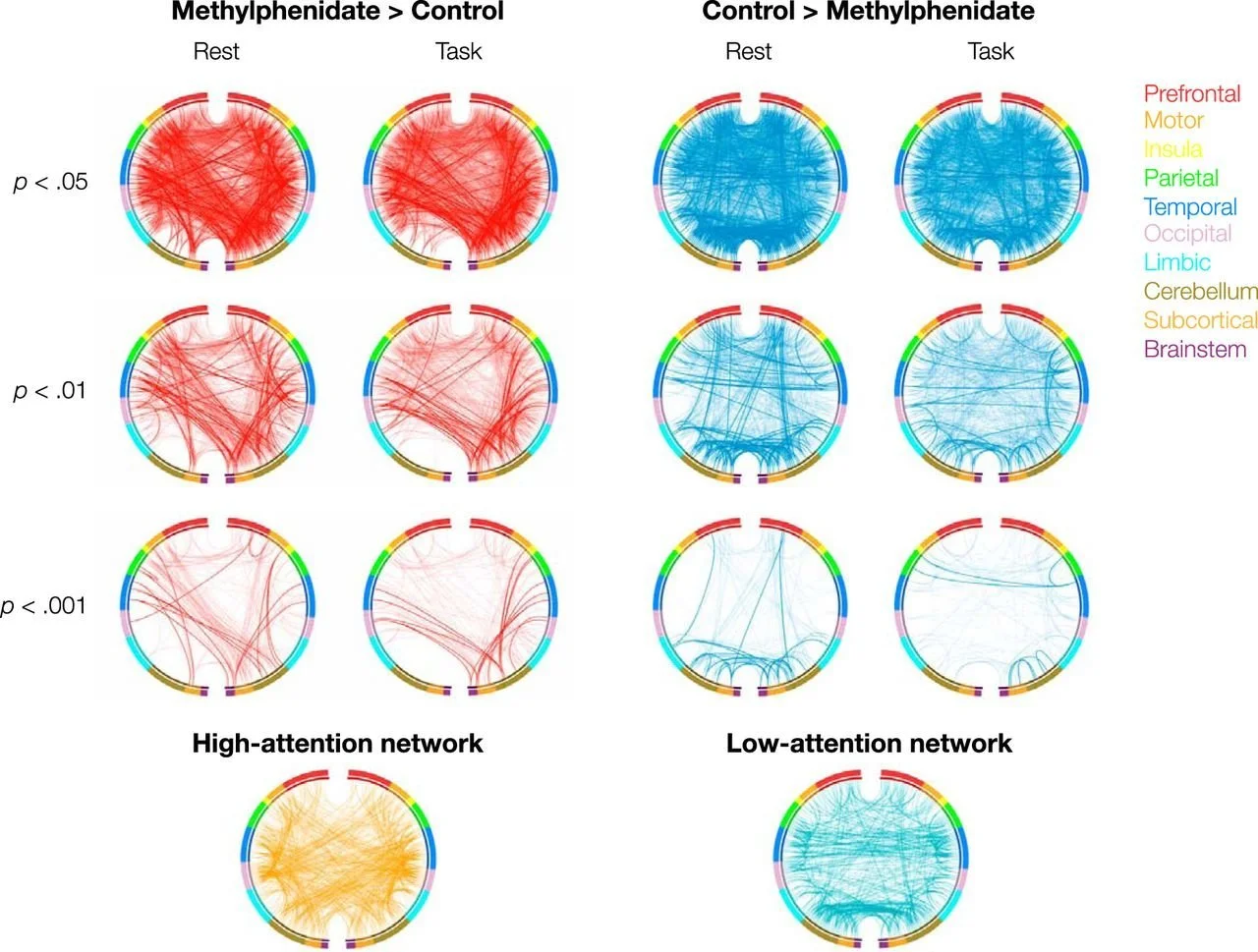
Methylphenidate does not create attention, but reorganises the brain so that attention networks can work better and distraction networks interfere less. The red lines show brain connections that increase with methylphenidate, especially in networks involved in attention and cognitive control. The blue lines show stronger connections without medication, associated with networks linked to lower attention or greater distraction. These changes are mainly seen in connections between the prefrontal cortex, parietal regions and the insula, key areas for attention, executive control and behavioural regulation.
Figure reproduced from: Rosenberg et al., J Neurosci. 2016 Sep 14;36(37):9547-57, under a Creative Commons CC BY 4.0 licence.
ADHD medication as a relational tool
For me, this is where things change. Because then medication stops being a passive sticking plaster and becomes a relational tool. Something that helps you listen better. To pause earlier, respond with a little more space, and realise that perhaps you were not lazy, chaotic, immature or morally defective. Perhaps you were trying to hold a demanding life with a nervous system that had been under pressure for far too long.
And this does not mean idealising medication. We need to speak clearly here too. ADHD medications are not completely free of risk, but when they are properly prescribed and monitored, the risks are usually considerably smaller than many people imagine. With methylphenidate, for example, what is most commonly monitored is pulse, blood pressure, appetite, sleep and mood changes.
In the UK, where I have lived for 32 years, the National Health Service, the NHS, notes that small increases in heart rate and blood pressure can occur, and that serious side effects are uncommon. In the United States, the National Institute of Mental Health, the NIMH, has also stated that stimulants are generally safe, and that the risk of dependence or abuse is low when they are used properly, as prescribed and under clinical supervision.
By contrast, the risks of living with untreated or insufficiently treated ADHD are often minimised far too much. And they are not small. ADHD is associated with greater suicidality, more psychiatric comorbidity, more functional difficulties and more accumulated suffering. In addition, recent and fairly robust observational studies have found that starting pharmacological treatment is associated with lower rates of suicidal behaviours, problematic substance use, traffic accidents, criminality and, in some analyses, lower overall mortality, especially from non-natural causes.
This does not prove a perfect causal relationship, but it does force us to abandon the simplistic idea that the major risk lies only in taking medication. It is more likely that years without support may have carried a much greater risk. ⁴ ⁵
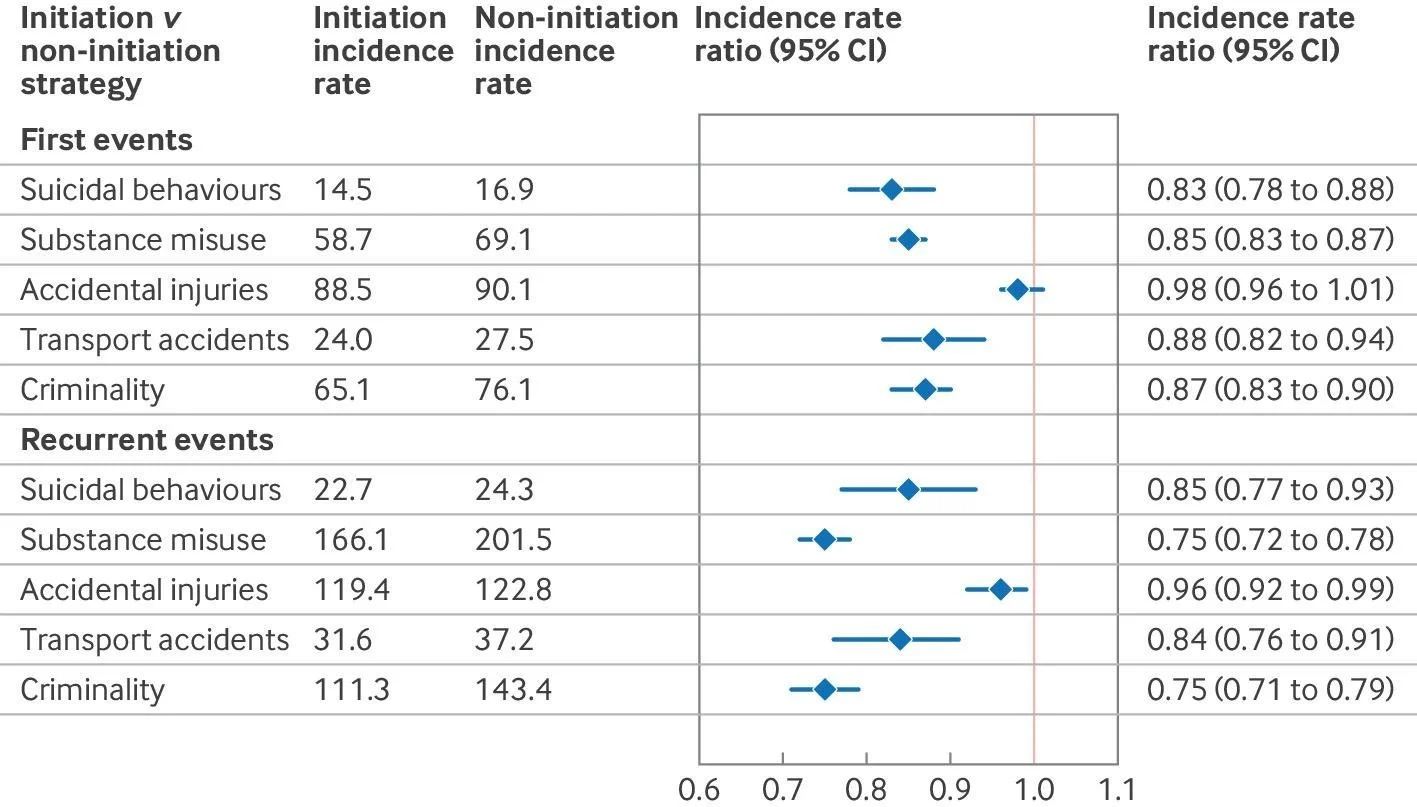
This graph shows that people with ADHD receiving pharmacological treatment have a lower risk of suicidal behaviours, substance misuse, transport accidents and criminality compared with people who are not medicated.
Overall, the results suggest that treating ADHD is associated with a significant reduction in several important health and safety risks over time. This goes beyond “performing better” or “concentrating more”. It is much less about that and much more about creating the breathing space I am talking about in this article.
Figure reproduced from: Zhang et al, BMJ. 2025 Aug 13;390:e083658, under a Creative Commons CC BY 4.0 licence.
ADHD meds open the door, but you still have to walk through it
It is also worth being honest about another point. Medication may help with some aspects of emotional dysregulation, and recent evidence points towards moderate benefits in this area, but that does not mean it will instantly erase years of hypervigilance, rejection sensitivity, relational trauma or self-abandonment. Some parts of that work still require something slower, more human and deeper. Therapy, body, rest, grief, a great deal of self-observation, and unlearning rhythms you are no longer aligned with so that you can learn new ones.
In fact, I did exactly what many people do. After several years on medication, I stopped taking it. There was a lot of self-stigma there. A great need to prove to myself that I could do it “properly”, in a more natural way. I thought supplements, food, exercise, meditation and discipline would be a purer option, more coherent, perhaps even more virtuous.
But there was a trap hidden inside that narrative. I had not yet understood that all those things do not disappear when you take medication. They remain valuable. And for some people, they work even better. With less internal battle. Less of that exhausting stress of wanting to exercise and not being able to start. Wanting to cook yourself something nourishing and ending up not eating again. Wanting to meditate and then feeling like you have failed even at trying to care for yourself.
Medication does not compete with these pillars. It can make them more accessible.
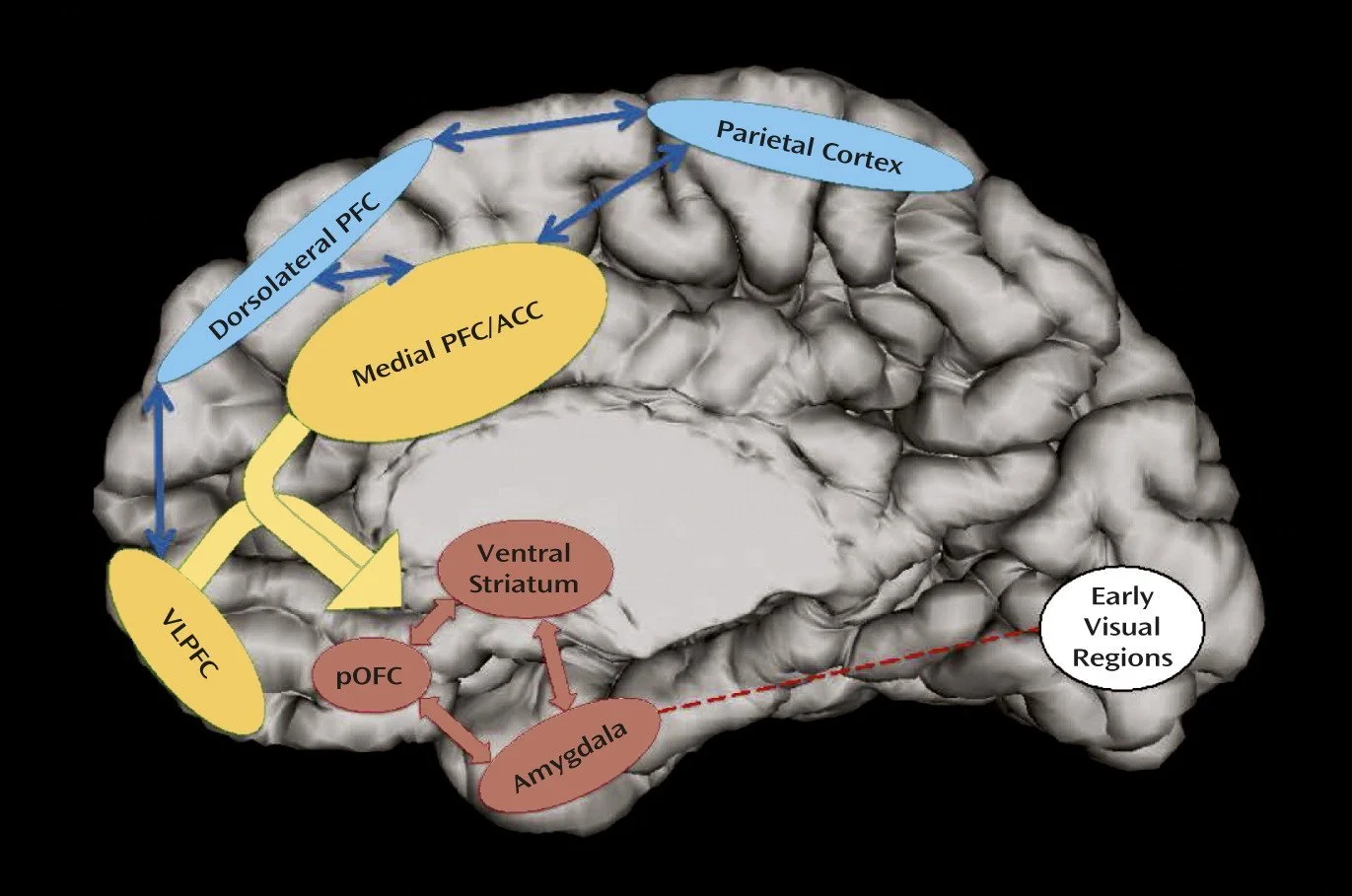
Emotional regulation depends on the dialogue between cognitive control networks, the prefrontal and parietal cortex, and emotional networks such as the amygdala and ventral striatum. Medication may help these networks coordinate more effectively, but a pill does not replace the full process of emotional regulation.
Figure reproduced from: Shaw et al., Am J Psychiatry. 2014 Mar;171(3):276-93, under a Creative Commons CC BY 4.0 licence.
And this is where something beautiful comes in: neuroplasticity
When we understand what supports us, practise it and repeat it, the brain learns. It leaves traces and strengthens pathways. Stimulants modulate dopaminergic and noradrenergic systems that participate in attention and learning, and recent reviews show that they also modify functional brain networks related to focus and self-regulation.
In fact, one study in adults found sustained changes in functional connectivity after four months of methylphenidate, without signs of neurobiological tolerance during that period. I would not use this to sell miracles. But I would use it to remember something important. Medication can create a more stable terrain so that repeated habits, rest, therapy, movement and listening to the body can leave a deeper imprint. ⁶ ⁷

When it comes to supplements, I also think it is important to step away from black-and-white thinking. There are interesting supplements that I will be writing about. Some, such as saffron, show promising results in small studies, even as an adjunct to methylphenidate. I have, in fact, taken it every day for years. But one thing is touching some potentially relevant mechanisms, and another very different thing is consistently reproducing the tangible clinical experience many people describe when a medication works well for them. The evidence for supplements remains much smaller, more heterogeneous and less predictable. That is why I do not like framing the conversation as supplements or medication, because it feels like a false dichotomy. It feels much more appropriate to build support rather than choose purity.
Perhaps, deep down, what I am talking about here is dignity
Leaving behind the idea that treatment should only be measured by how much you produce. Beginning to measure it also by how much less you suffer. By how much less you fight with yourself. By how much easier it becomes to move closer to your values. By how much more inhabitable your body becomes. By how much less frightened you feel of being who you are. Medication on its own will not give you a meaningful life, but it may help you hold life more steadily while you learn to listen to it.
And so we return to the starting point. After reading hundreds of high-quality clinical studies, but also after feeling in my own body the difference between being medicated and not being medicated, there is something that, for me, no longer leaves much room for doubt. Medication is not the goal. It is the buffer between reality hitting you in the face and your ability to react to it in a way that is more aligned with the person you want to be. It is not a magic solution. It does not erase your history. It does not do for you the emotional, relational and existential work you may have needed for years. But it can give you something profoundly valuable: space. Space to breathe. Space to choose better. Space to begin building a kinder relationship with yourself. And when you have spent too long living at the edge of yourself, that space can be the beginning of everything. None of this replaces an individual assessment with your doctor or prescriber. The decision to take medication, adjust a dose, change medication or not take it at all should always be clinical, shared and personalised. But it should also take into account your history, your rhythms, your body and your emotional needs. Because when all of that enters the conversation, deciding stops feeling like a battle and starts to look more like a form of care.
And remember something important. Your value as a human being does not depend on whether you take medication or not. Do not allow prejudice or stigma around medication to decide for you. Make the decision that makes sense at this moment in your life, with the information and support you have now. If later on you need to change your mind, that is also okay. Neuroplasticity does not only speak to how the brain changes, but also to our capacity to think with flexibility. Being able to review decisions, adjust them and adapt them to our new circumstances is not a sign of weakness, but a form of health. And sometimes, even an expression of personal growth.
With care,

The content of this article is for educational and informational purposes only. It is not intended to replace medical advice, diagnosis, psychotherapy or individualised treatment from a qualified professional. If you are making decisions about medication, supplements, mental health, sleep or any other aspect of your care, please speak with your doctor, prescriber and/or therapist first.
If you are navigating these decisions in your own life and feel it would help to have someone consider them with you calmly, my ADHD & Neurodivergence Wellbeing page explains how I work one-to-one.
References: the science informing this article
Bellato, A., Perrott, N. J., Marzulli, L., Parlatini, V., Coghill, D., & Cortese, S. (2025). Systematic Review and Meta-Analysis: Effects of Pharmacological Treatment for Attention-Deficit/Hyperactivity Disorder on Quality of Life. Journal of the American Academy of Child and Adolescent Psychiatry, 64(3), 346–361. https://doi.org/10.1016/j.jaac.2024.05.023.
Notes: This systematic review and meta-analysis of 17 randomised clinical trials, including 5,388 participants, found that ADHD medications, including stimulants such as amphetamines and methylphenidate and non-stimulants such as atomoxetine, significantly improve quality of life compared with placebo.
The most important point to highlight from this study is that the results suggest medication does not only reduce core ADHD symptoms, but also produces moderate improvements in quality of life, reinforcing its role within a comprehensive therapeutic approach. This goes beyond personal opinions about whether medication should or should not be used, and aligns with the scientific evidence itself.
National Institute for Health and Care Excellence. (2018, actualizado 2019). Attention deficit hyperactivity disorder: Diagnosis and management (NICE Guideline NG87).https://www.nice.org.uk/guidance/ng87
Notes: This NICE clinical guideline from the UK sets out evidence-based recommendations for the diagnosis and treatment of ADHD across the lifespan. It highlights that pharmacological treatment, including methylphenidate and lisdexamfetamine in adults, should be integrated within a broader and personalised therapeutic plan.
NHS England. (2024). Report of the independent ADHD taskforce: Part 1.https://www.england.nhs.uk/long-read/report-of-the-independent-adhd-taskforce-part-1/
Notes: This independent report commissioned by NHS England reviews the evidence on the impact of ADHD across the lifespan and the current limitations in access to diagnosis and treatment within the healthcare system. It highlights that untreated ADHD is associated with a higher risk of mental health problems, suicidality, social difficulties and adverse functional outcomes, underlining the importance of improving access to effective clinical interventions.
Zhang, L., Zhu, N., Sjölander, A., Nourredine, M., Li, L., Garcia-Argibay, M., Kuja-Halkola, R., Brikell, I., Lichtenstein, P., D'Onofrio, B. M., Larsson, H., Cortese, S., & Chang, Z. (2025). ADHD drug treatment and risk of suicidal behaviours, substance misuse, accidental injuries, transport accidents, and criminality: emulation of target trials. BMJ (Clinical research ed.), 390, e083658. https://doi.org/10.1136/bmj-2024-083658
Notes: This population-based study, which emulates clinical trials using large-scale observational data, found that pharmacological treatment for ADHD is associated with a reduced risk of suicidal behaviours, substance misuse, accidental injuries, transport accidents and criminality. The findings, published in the British Medical Journal, suggest that medication may not only reduce core ADHD symptoms, but also reduce important risks to health and social functioning when ADHD is treated according to the person’s needs.
Balazs, J., & Kereszteny, A. (2017). Attention-deficit/hyperactivity disorder and suicide: A systematic review. World journal of psychiatry, 7(1), 44–59. https://doi.org/10.5498/wjp.v7.i1.44
Notes: This systematic review, which analyses 26 studies, shows that ADHD is associated with a significantly higher risk of suicidal ideation and suicide attempts, helping us understand the impact of ADHD when it is not recognised or adequately treated.
Parlatini, V., Bellato, A., Murphy, D., & Cortese, S. (2024). From neurons to brain networks, pharmacodynamics of stimulant medication for ADHD. Neuroscience and biobehavioral reviews, 164, 105841. https://doi.org/10.1016/j.neubiorev.2024.105841
Notes: This study reviews how stimulants used in ADHD, including methylphenidate and amphetamines, act from the neurochemical level through to the reorganisation of brain networks involved in attention, cognitive control and motivation. I find this article relevant because it shows that the effects of these medications are not limited to increasing neurotransmitters, but also modulate communication between brain networks that are key for behavioural regulation.
Vansina, E., Douw, L., Kaiser, A., van der Pal, Z., Boucherie, D. E., De Vries, T. J., Pattij, T., Cohen, J. R., Hoekstra, P. J., Reneman, L., & Schrantee, A. (2025). Effects of 4-Month Methylphenidate Treatment on Functional Connectivity in Attention-Deficit Hyperactivity Disorder. medRxiv : the preprint server for health sciences, 2025.08.27.25334547. https://doi.org/10.1101/2025.08.27.25334547
Notes: This study examines how four months of methylphenidate treatment is associated with changes in the functional connectivity of brain networks involved in attention and cognitive control in people with ADHD. Although the findings suggest a reorganisation of communication between brain networks after treatment, the study is still a preprint and has not yet been peer reviewed. Even so, I find it very interesting, so I am following it closely and hope its publication is confirmed soon.
The results are also consistent with older published studies, such as the 2014 systematic review by Rubia et al. (Rubia, K., Alegria, A. A., Cubillo, A. I., Smith, A. B., Brammer, M. J., & Radua, J. (2014). Effects of stimulants on brain function in attention-deficit/hyperactivity disorder: a systematic review and meta-analysis. Biological Psychiatry, 76(8), 616-628. https://doi.org/10.1016/j.biopsych.2013.10.016). This neuroimaging study showed that methylphenidate normalises patterns of functional connectivity between brain networks involved in executive control and attention in people with ADHD. The results suggest that the medication may reorganise communication between brain networks that support cognitive and behavioural regulation.
There is also the 2005 study by Silk et al. (Silk, T., Vance, A., Rinehart, N., Egan, G., O’Boyle, M., Bradshaw, J. L., & Cunnington, R. (2005). Fronto-parietal activation in attention-deficit hyperactivity disorder, combined type: functional magnetic resonance imaging study. The British Journal of Psychiatry, 187, 282-283. https://doi.org/10.1192/bjp.187.3.282), another neuroimaging study using functional magnetic resonance imaging, which found that methylphenidate increases activation and connectivity in frontoparietal networks associated with working memory and executive control in ADHD.
The findings of both studies support the idea that pharmacological treatment may improve the functioning of brain networks that are key not only for attention, but also for emotional and cognitive regulation.
Join the conversation
Share a thought, reflection or question.
Please keep this space thoughtful, respectful and kind. Thank you.